If it seems like you’ve been hearing more about horse stifles lately, it’s because you probably have. This hind limb joint—one of the largest and most complex in the horse’s entire body–has been the subject of increased attention from researchers, joint specialists and front-line field veterinarians in recent years. The stifle is the “it” joint right now, and with good reason.
“With advances in imaging technology, it’s easier than it has ever been to diagnose and treat the problems that arise in the stifle,” says David Frisbie, DVM, PhD, of Colorado State University. “Twenty years ago nobody really blocked stifles (for diagnostics), and up until about 10 years ago nobody really bothered treating them. Unless you were a surgeon and willing to open them up and look around, you just didn’t feel like there were many viable options.”
Now, however, stifles aren’t nearly as vexing. “We’ve just gotten so much better at dealing with them,” says Gary Baxter, VMD, MS, of the University of Georgia. “And as a result, more veterinarians are willing to go looking. You may be hearing more about stifle lameness lately, but it’s not because more horses have stifle injuries. It’s just that we are better able to recognize and diagnose the problem and initiate treatment. Before, these horses would have an ‘unknown’ lameness.”
These advances in diagnostic and treatment techniques are self-perpetuating as they inspire and allow inquisitive researchers to learn even more. “It may sound silly, but the stifle is exciting,” says Frisbie. “We know so much about the other joints that they are kind of boring and routine now. And when things are boring and routine, we move on to the next big adventure, and currently—for veterinarians and surgeons like myself—that’s the stifle.”
Sum of the parts
Although horsemen refer to the stifle as if it were a single joint, it’s actually a three-for-one deal with lots of extras thrown in. Wrapping your mind around the anatomy of the stifle joint can take a few minutes, but it’s important for understanding the diagnostic and treatment challenges it presents.
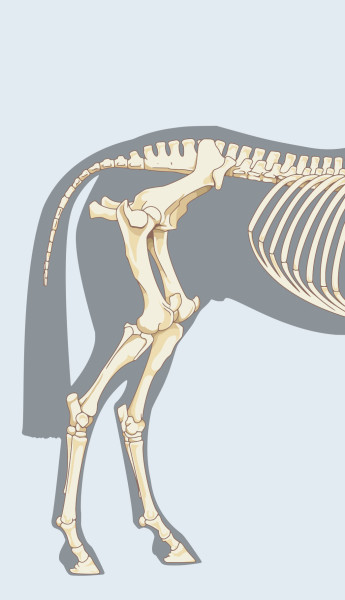
The stifle is the area where the tibia, the bone that forms the gaskin, meets the femur, the bone that extends upward to the hip. The stifle is analogous to the human knee: When you pick up a horse’s hind leg, the joint bends forward, just as your knee does as you climb a staircase.
Looking at the bones themselves, you’ll see things get a bit more complicated. There is a large cleft—called a “septum”—in the lower end of the femur where it meets the upper end of the tibia. This cleft creates two distinct joints at that junction. These joints are right next to each other and flex in the same direction and at the same time, so functionally they appear to be one. The innermost of these is called the “medial femoral tibial joint” and the outer one is the “lateral femoral tibial joint.”
Sitting in each of these femoral tibial joints is a structure called a meniscus—two menisci per stifle. These thick pads of fibrocartilage are “much stronger than regular cartilage,” says Baxter. “They are more like a combination of cartilage and ligament tissue together.” Menisci disperse the horse’s body weight throughout the joint and reduce friction as the horse moves.
“You can think of each meniscus as shaped sort of like a teacup,” explains Frisbie. “The bottom side of the teacup sits on the tibia and the rounded end of the femur sits inside the cup. The meniscus holds the femur in place while helping it glide as the joint flexes. If you understand the role of ball bearings in mechanics, it’s very similar to that.”
The third joint of the stifle is formed at the meeting of the patella (analogous to the human kneecap) and the bottom of the femur bone. “I think of the patella joint as the ‘front’ stifle joint and the femoral tibial joints as the two ‘behind’ it, even though they aren’t exactly aligned,” says Baxter.

The patella joint isn’t particularly mobile, but it allows the shield-shaped bone to “float” above the femur, protecting it and—most important—acting as an anchor point for the three patellar ligaments: The “medial patellar ligament” is on the inside of the joint; the “middle patellar ligament” runs down the face of the joint, and the “lateral patellar ligament” is on the outside. These ligaments attach the patella to the tibia, the lower bone of the stifle. If you’re familiar with the condition known as “sticking” or “locking” stifles, technically called “upward fixation of the patella,” you’re familiar with how complex and finicky this arrangement of bones and ligaments can be.
Click here to read about research into treatment of locking stifles.
Two other short, thick ligaments—the medial and lateral collateral ligaments—join the femur and tibia bones on the outside edges of the joint. Two more ligaments, buried deep in the cleft area, are the anterior and posterior cruciate ligaments. These help to stabilize the joint as the horse works.
Add to this collection of bones, ligaments and menisci the fluids and cartilage found in other joints, and you’ve got one of the most complex areas in the equine body. “The stifle is a highly mobile, weight-bearing joint,” says Baxter. “It has lots of components that all have to work together seamlessly with each stride. The only other area that might be as complex, musculoskeletally speaking, is the shoulder.”
The stifle joint is designed for a limited type of motion, and problems arise when it moves in other directions. “The way the stifle joints are set up, the anatomy and geometry are optimized for going backward and forward, not side to side,” says Frisbie. “When things start moving sideways or twisting, you start to get injuries, both acute and chronic.”
A horse’s job description greatly influences his risk of stifle injury. “Disciplines where you see more sideways motion, like cutting, will have more stifle injuries as a result,” says Frisbie. “Horses who jump a lot can also have stifle injuries because of the forces involved in pushing up and over a large fence, particularly on footing that might be slick. There was a demographic paper that reported that some 40 percent of horses who event have some type of stifle issue. I’d say that horses in Western performance disciplines are likely on par with that or higher.”
But any horse can injure a stifle. “A horse could certainly slip in the paddock while playing and pull a ligament,” says Baxter. “And years of riding and concussion of any type can take a toll on the joint, leading to arthritis, which is simply a long-term chronic injury.”
Diagnostic advances
Stifle injuries can be difficult to detect. Unlike a hoof abscess or a bowed tendon, stifle problems don’t have a “tell” as reliable as a distinct head bob or limp. “You can sometimes see it in how they bear weight in the stance and push-off phase of a stride,” says Frisbie. “The horse may drop down or ‘give’ in the stifle as that limb bears weight.” But, he says, that’s not always reliable.
“Just the other day I saw a horse where the trainer, who was a very skilled professional, told me, ‘It feels like a stifle problem,’” he continues. “And when I saw the horse move, I thought, ‘Yep, that looks like a stifle problem.’ But then the horse blocked out sound in an entirely different joint. There are some rules of thumb but no clear hallmarks of stifle lameness.”
Baxter adds that what appears to be a behavior or training issue might actually be stifle lameness. “There are some stifle problems that, early on, show up only as the horse being reluctant to work,” he says. “I’ve seen some younger horses with hurting stifles that aren’t willing to turn as quickly and sharply as they did before.”
Investigating a suspected stifle injury will begin with a visual exam. “Acute stifle injuries are usually going to have some effusion [swelling] associated with them,” says Baxter. “It’s not something an owner might notice, but if you’ve seen enough and know where to look, it’s something you can often spot right away.”
Whether an injury to the stifle involves bone, ligament, meniscus or other structures, chances are it’s on the inside of the limb. “This is a result of how the horse bears weight on the entire limb, not necessarily specific to the stifle,” says Baxter. “In general, anytime you have a problem in any limb joint—pastern arthritis or bog spavin in the hock—it’s more likely on the medial side.”
After an initial visual exam, flexion tests and watching the horse move in-hand and perhaps under saddle, a veterinarian who suspects a stifle injury may “block” that area with a numbing agent. “Personally, I’ll block all three joints at the same time,” says Frisbie. “Then, if the horse goes sound, I know it’s that area, and I’ll use imaging to look closer. If I don’t see anything with imaging, I’ll go back and start blocking each of the joints in the stifle one at a time.”
The difficulty in blocking individual joints, Frisbie explains, is that they can “communicate” with each other, so blocking one can affect the other two. “You can never be 100 percent certain you’ve isolated it to just one joint,” he says. “Even when you look surgically, it’s not always clear where the issue is.”
After blocking a joint, a veterinarian will turn to imaging technology, using radiographs, ultrasound or both in the suspected areas. “Some areas of the joint you can see radiographically, others are better seen with ultrasound, so veterinarians will often use some combination of the two, looking for anything unusual,” says Baxter. “Of course, radiography is primarily going to show you bone problems and the ultrasound will show you soft tissue, so that’s also a consideration.”
The influence of improved ultrasound technology on the management of stifle injuries has been profound. “Our ability to make a definitive diagnosis of stifle injuries without surgery has really emerged only in the past decade,” says Frisbie. “Advances in ultrasound account for much of that.”
If, after radiographs and ultrasound are done, the veterinarian still wants a closer look, arthroscopy is an option. In this diagnostic procedure, a small camera attached to a flexible tube is inserted into the joint area and transmits images to a monitor. “You can see quite a bit,” says Baxter. “And certain areas of the stifle, like the cruciate ligaments, can be seen best with arthroscopy.”
Conventional arthroscopy qualifies as surgery, requiring that the horse be anesthetized and leaving incisions behind to heal. A new development, however, is needle arthroscopy, which uses a scope that is the width of a hypodermic needle. “I started using this scope on stifles about three years ago,” says Frisbie. “Now I can look around inside these horses while they are still standing and see injuries that aren’t yet visible on radiographs. It’s opening up a whole new realm of diagnosing horses early, while the changes to the joint are less severe and much more manageable.”
Treating common injuries
Using all of these diagnostic techniques, a veterinarian can—in most cases—make a definitive diagnosis of a stifle injury. “It’s always better to know what the problem is,” says Baxter. “We might not always be able to fix it, but you can’t even try if you don’t have a diagnosis.” Here are just a few of the possible causes of stifle lameness:
Meniscal tears, usually caused by shearing and twisting forces, are one of the more common acute injuries of the stifle. The meniscus itself can tear, or the ligament that attaches it to the tibia can tear, or both.
“Much of the seriousness of the injury is related to how badly damaged the meniscus is,” says Baxter. “A true tear can cause considerable lameness. At the other end of the spectrum, a little fraying of the meniscus may not cause much of a problem in terms of lameness.”
The location of the tear on the meniscus itself also influences the severity of injury and prognosis. “If the tear is in an area you can access surgically, you may be able to go in and debride any frayed areas or even suture it back together,” says Baxter. “But if the injury is under the condyle of the bone, you may not be able to see it, much less reach it for treatment.” Of course, rest and anti-inflammatory medications can help, but menisci typically don’t heal well on their own. If the horse has had repeated injuries, the prognosis for long-term soundness without more therapeutic intervention is very guarded.
That said, modern stem cell therapy is healing meniscal injuries that just a few years ago would have been considered hopeless, says Frisbie. “The largest set of horses that have been reported on had a 6 percent chance of going back to work with a severe or grade 3 meniscal tear after surgery alone. This number has been increased two to four times with the addition of stem cell therapy in conjunction with the surgery,” he says. Strained or torn ligaments around the stifle aren’t nearly as common in horses as you might expect. “You hear of professional athletes—football players especially—tearing through their cruciate ligaments on a single bad play. That’s the dreaded ‘ACL’ injury that can end a career,” says Frisbie. “Horses aren’t as likely to injure that ligament so dramatically, but then again, we don’t play contact sports with horses.”
Your experience with dogs may not be applicable either: “In dogs [ACL injuries] can be degenerative, with partial tears, but we haven’t recognized that type of injury in horses. I’m not saying it can’t happen, but it’s definitely not as common,” says Baxter.
There are, however, ways horses can injure one of the many other ligaments of the stifle, such as the collateral ligaments. “If a horse gets its foot caught, this can cause a severe traumatic injury, pulling those ligaments,” says Baxter. “The collateral ligaments are very stout, and if they are significantly injured you can generally diagnose this either with a physical exam or ultrasound.”
Treating ligament injuries in the stifle is similar to how they would be managed elsewhere in the body. “Rest, anti-inflammatory medications and maybe stem cells if we can locate and access the damaged area,” says Frisbie. “These are all things we can try, and if we’ve caught it early and the injury isn’t too severe, they might work, and the horse doesn’t look back.”
Arthritis can develop in the stifle, just as it does in any other joint in the body. One of the earliest signs of this degenerative disease may be subtle lameness combined with osteophytes seen on stifle radiographs. With chronic arthritis, subchondral bone cysts—pockets of fluid/soft tissue that form in the bone underneath the cartilage—can develop in weight-bearing areas of the joint. “These develop from concussive forces,” says Baxter. “There are many reported methods of treating these cysts, but the problem is they don’t tend to fill in with normal bone. If you take out the contents surgically, you’ve taken out cartilage along the joint, and in a weight-bearing joint like the stifle, that can cause problems. Some horses do OK, but they generally don’t do as well as we’d like.”
Other treatment options for bone cysts include creating microfractures at the site to encourage the body to heal the area, steroid injections into the cyst and even filling the defects in with bone cells and biologics in the hopes they will regenerate a new surface. “Generally, all of these tend to work best in younger animals,” says Baxter. “Traumatic injuries that are older—like arthritis tends to be—are less responsive.”
Supplements, anti-inflammatories and injections can help control arthritis of the stifle as they would in any other joint, but Baxter doesn’t mince words when it comes to the long-term prognosis. “I think, in general, arthritis in the stifle is tough. It’s tough in any joint, but the weight-bearing surface of the medial femoral tibial joint—where arthritis is likely to develop—is one of the largest surface areas in the horse’s body. We can inject the stifle like we do any joint, and we do that often. It’s just less likely that we will see the results we want.”
Overall, says Baxter, the prognosis for minor and even moderate stifle injuries is good if they are recognized early. “Horses are usually pretty good at telling us when they have a problem with their stifles. It would be very unusual for a horse to have a major issue with no outward indications like swelling or lameness. So if we pay attention, we can catch them early.”
An early diagnosis calls for early intervention, says Frisbie. “If I had one criticism it would be that we, surgeons and veterinarians, still tend to not work on stifles on a first-line basis. We tend to inject and rest for six months to a year, hoping it will help. The trouble is, if it doesn’t, we’ve now got an older, more chronic injury to contend with, and that’s much more difficult. We should not only treat but diagnose the problem as early as possible.”
If the stifle joint is an unexplored frontier in equine joints, it won’t be for long. As curious veterinarians embrace the latest technologies, what was once a daunting proposition—diagnosing and treating injuries to the joint—is becoming achievable, and maybe one day, even routine.
This article first appeared in EQUUS issue #439.
Don’t miss out! With the free weekly EQUUS newsletter, you’ll get the latest horse health information delivered right to your in basket! If you’re not already receiving the EQUUS newsletter, click here to sign up. It’s *free*!